How AI Is Reshaping Population Health & UM
There’s a quiet transformation happening inside health plans, provider organizations, and managed care companies. It doesn’t show up on patient-facing apps or hospital lobby screens — it’s happening in the back-office systems that decide who gets a care manager call, which claims get reviewed, and how quickly a prior authorization moves through the queue. At the center of this shift is artificial intelligence, and its impact on both population health strategy and utilization management is becoming hard to ignore.
For organizations still relying on manual processes and legacy platforms, the gap is widening. The question isn’t really whether to modernize anymore — it’s how fast, and with what tools.
Population Health Has a Data Problem — AI Is Fixing It
Managing the health of a large population has always required sorting through enormous volumes of data — claims, labs, pharmacy records, social determinants, risk scores, and more. For years, that sorting happened manually or through basic rules-based systems that couldn’t adapt, personalize, or predict.
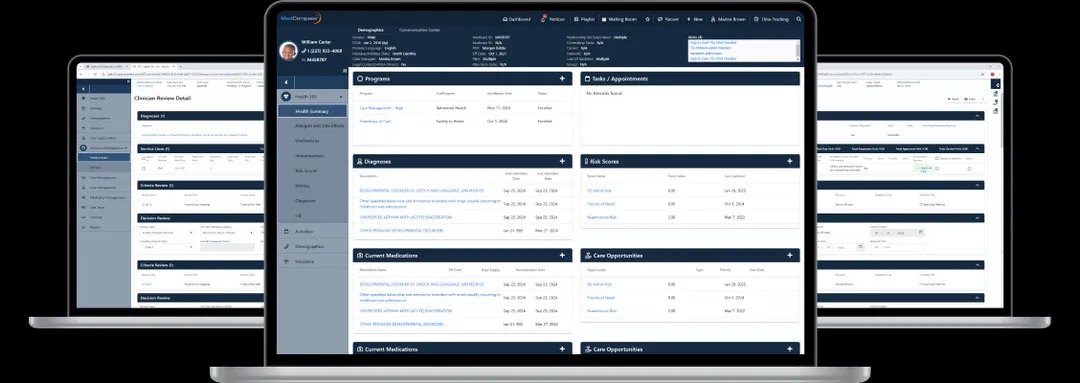
That’s precisely the gap that AI population health management software is built to close. Rather than waiting for a patient to show up in crisis, this kind of platform works continuously in the background — analyzing patterns, stratifying risk, and surfacing the individuals most likely to deteriorate if no one intervenes. It’s a fundamentally different approach to care management: predictive rather than reactive, targeted rather than broad.
What makes AI-driven population health tools stand apart from older analytics platforms is their ability to learn. A static risk model built in 2019 isn’t going to reflect today’s patient population accurately. Machine learning models update as new data flows in, meaning the risk stratification your team acts on today is informed by what’s actually happening now — not by a snapshot from three years ago.
For care managers, this changes the daily workflow in a meaningful way. Instead of pulling reports and manually triaging a list of high-risk members, the AI population health management software does that prioritization automatically. Care managers start their day knowing exactly who needs outreach, why, and what intervention is most likely to help — freeing up time for the actual clinical work rather than the administrative overhead.
Utilization Management: Still Too Manual in Most Organizations
On the utilization management side, the picture looks remarkably similar. Most UM teams are dealing with a volume problem — prior authorization requests, concurrent reviews, discharge planning, appeals — all of it landing in queues that humans have to sort, prioritize, and process. Even with skilled clinical staff, the backlog creates delays. And delays in UM aren’t just an operational inconvenience; they affect patient access to care and expose organizations to compliance risk.
Structured utilization management workflows address this by replacing ad hoc, inconsistent processes with standardized, technology-supported pathways. Every request moves through the same logical sequence. Clinical criteria are applied consistently. Documentation requirements are built into the workflow so nothing gets missed. And when a case needs escalation — to a physician advisor, for example — that handoff happens automatically rather than depending on someone remembering to route it.
The impact on turnaround time alone is significant. Organizations that modernize their utilization management workflows typically see faster authorization decisions, fewer incomplete submissions, and a measurable drop in administrative rework. When staff aren’t hunting down missing information or re-routing cases that fell through the cracks, they have more capacity for the complex reviews that actually require clinical judgment.
There’s also a compliance dimension that often gets overlooked. Regulatory requirements around UM — timelines, documentation, appeal rights — are strict, and inconsistent manual processes are a common source of audit findings. Structured utilization management workflows create a built-in audit trail: every decision, every touchpoint, every escalation is logged in a way that’s easy to review and report on.
When Population Health and UM Work Together
In many organizations, population health and utilization management operate as separate departments with separate tools. That separation creates blind spots. A member flagged as high-risk in the population health platform might simultaneously have a prior authorization stuck in the UM queue — and neither team knows what the other is doing.
When AI population health management software and structured utilization management workflows are connected within the same ecosystem, that kind of disconnect disappears. The care manager working with a high-risk diabetic patient can see their active authorizations. The UM nurse reviewing a hospital admission request can see the patient’s care plan and recent risk score. Decisions get made with complete context rather than a partial view.
This integration also creates feedback loops that improve performance over time. If certain utilization patterns consistently appear in high-risk populations, the AI can surface those connections. If particular intervention types are leading to avoidable admissions in the UM data, that insight feeds back into the population health risk model. The two systems make each other smarter.
What This Means for Health Plans and Care Organizations
For health plans, the business case is straightforward. Better population health management reduces avoidable utilization — ED visits, preventable admissions, duplicative testing. More efficient utilization management workflows reduce administrative cost and improve member experience. Both contribute directly to the financial and quality metrics that matter: medical loss ratio, star ratings, HEDIS scores.
For provider-led organizations taking on risk, the stakes are even higher. When you’re accountable for outcomes, having the right intelligence at the right moment isn’t a nice-to-have — it’s what determines whether you’re managing cost effectively or absorbing losses you didn’t anticipate.
And for the care teams doing the actual work — the nurses, care managers, UM reviewers, and physician advisors — better tools mean less time on administrative busywork and more time on the clinical decisions that require human expertise. That’s not just an efficiency argument. It’s a workforce sustainability argument at a time when clinical burnout is a serious concern across the industry.
The Takeaway
AI is not a silver bullet, and no platform replaces the clinical judgment of skilled professionals. But the organizations getting the best results right now are the ones that have stopped treating technology as a documentation tool and started treating it as a decision-support engine. That means investing in AI population health management software that actually predicts and prioritizes, and building utilization management workflows that are consistent, auditable, and connected to the broader care picture.
The complexity of managing population health and utilization at scale isn’t going away. But with the right tools, it becomes a problem organizations can stay ahead of — rather than constantly trying to catch up.
AssureCare’s OptiMaizer and Utilization Management solutions are built for exactly these challenges. Learn more at assurecare.com.
Share this content:








Post Comment